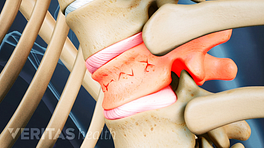
If you have been diagnosed as having a fracture, the doctor tells you you do have a vertebral fracture, not necessarily to do anything invasive in terms of treatment. Most fractures, if they are simple small fractures, will heal. Some pain medicine for a few days to a few weeks may be all that’s necessary. If the pain doesn’t get better or if it is so disabling you can’t function, there are certainly options from a minor surgical standpoint to do minimally invasive procedures to help bolster the strength of the vertebrae in order to relieve pain and to prevent any further collapse. We generally recommend if you have been diagnosed as having a fracture and you are not being treated surgically early on, which is common, to have an x-ray relatively frequently over the first few weeks just to make sure that things aren’t collapsing in some unacceptable position because many fractures can cause you to bend forward and have difficulty standing up and can be a progressive deformity if other fractures happen as well and that can have problems with standing and walking, in terms of pain, and can even in the long run result in breathing problems.
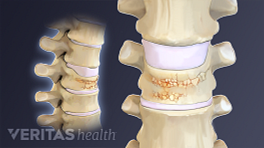
If the pain is bad enough to warrant some type of surgical treatment, the two most common types of procedures that are done are commonly called vertebroplasty or kyphoplasty. Now those are just terms and both of them refer to procedures where through small little needle holes in the skin, cement is injected into the vertebrae allowing for the fracture fragments of the vertebrae to congeal together and that helps provide immediate stability and relieve pain.
The difference is that in vertebroplasty the cement is put in in a fairly wet fashion and allowed to interdigitate among all of the different fracture fragments. And the position that the spine is in is the position that it stays in. Although if its a fresh fracture it certainly may be correctable by positioning of the patient before any cement is injected.
With kyphoplasty a special balloon device is inserted into the vertebrae and expanded and that provides some reconstitution of the height of the vertebrae and potentially correction of some angulation or collapsing or wedging of the vertebrae. And then within that defect within the middle of the vertebra a thicker cement is put in but also through a very minimally invasive way to fill that void again providing some immediate relief but also potentially correcting any deformity or collapse of the vertebrae.
Articles Related to this Video: