Lumbar facet joint disorders most commonly cause lower back pain that is characterized by a localized ache with some degree of stiffness. This pain is usually worse in the morning or after periods of inactivity. In case of spinal nerve root impingement, radicular leg pain (sciatica) may occur.
Several signs and symptoms of facet joint disorders may be similar to other lower back conditions, such as degenerative disc disease. These conditions also typically occur together, causing overlapping symptoms, which tends to make the diagnostic process more challenging.
In This Article:
- Facet Joint Disorders and Back Pain
- Causes of Lumbar Facet Joint Disorders
- Symptoms and Diagnosis of Facet Joint Disorders
- Treatment Options for Facet Joint Disorders
- Surgery for Lumbar Facet Joint Disorders
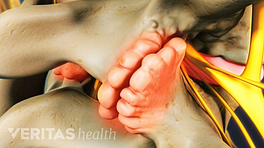
Symptoms of Lumbar Facet Joint Disorders
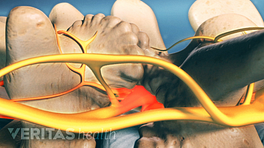
Nerve compression near the lumbar facets leads to sciatica.
Depending on the number of facets affected, the severity of the condition, and the possible involvement of a nearby nerve root, one or more of the following signs and symptoms may occur:
- Localized pain. A dull ache is typically present in the lower back. 1 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009. , 2 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009.
- Referred pain. The pain may be referred to the buttocks, hips, thighs, or knees, rarely extending below the knee. 1 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009. , 2 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009. Pain may also be referred to the abdomen and/or pelvis. 3 Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x This type of pain is usually caused by facet arthritis and is experienced as a distinct discomfort, typically characterized by a dull ache.
- Radiating pain. If a spinal nerve is irritated or compressed at the facet joint (such as from a facet bone spur), a sharp, shooting pain (sciatica) may radiate into the buttock, thigh, leg, and/or foot. Muscle weakness and fatigue may also occur in the affected leg.
- Tenderness on palpation. The pain may become more pronounced when the area over the affected facet in the lower back is gently pressed.
- Effect of posture and activity. The pain is usually worse in the morning, after long periods of inactivity, after heavy exercise, and/or while rotating or bending the spine backward. Prolonged sitting, such as driving a car, may also worsen the pain. The pain may be relieved while bending forward. 1 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009. , 2 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009.
- Stiffness. If the lumbar facet pain is due to arthritic conditions, stiffness may be present in the joint, typically felt more in the mornings or after a period of long rest, and is usually relieved after resuming physical activity.
- Crepitus. Arthritic changes in the facets may cause a feeling of grinding or grating in the joints upon movement.
If a single facet on one side of the spine is affected, the pain may be localized to one side of the lower back and thigh. Pain may occur on both sides (bilaterally) if both facets at a spinal segment are affected.
Diagnosis of Lumbar Facet Joint Disorders
A combination of clinical evaluation and medical imaging and/or diagnostic injection tests are usually considered to diagnose facet joint pain.
The initial step usually involves a doctor’s visit. The physical evaluation is likely to include multiple elements of a comprehensive exam.
Patient history
The doctor reviews the patient’s main complaints and asks about the onset of pain; duration and types of signs and symptoms; concomitant medical conditions; and drug and/or surgical history.
Medical exam
The doctor may gently palpate (feel) the lower back to check for tender spots and muscle reflex activity in the legs to rule out possible nerve dysfunction. A medical exam may include some combination of the following tests:
- Visual inspection of the overall posture and skin overlying the affected area
- Hands-on inspection by palpating for tender areas and muscle spasm
- Range of motion tests to check mobility and alignment of the involved joints
- Segmental examination to check each spinal segment for proper motion
- Neurological examination, including tests of muscle strength, skin sensation, and reflexes
If a clinical diagnosis of lumbar facet joint pain is suspected, first-line treatment options, such as medication, physical therapy, and spinal manipulation, may be advised. In general, diagnostic imaging and/or injection tests are not needed to treat and help resolve an episode of pain. If the first-line treatments are unsuccessful, then imaging and possibly injections may be recommended.
Medical imaging tests

MRI scans help distinguish a chronic condition from an acute problem in certain situations.
Standard radiographs, magnetic resonance imaging (MRI), computed tomography (CT) scans, and other specialized tests may be used to check the facet joint and adjacent structures.
- Standard radiographs may show bony changes and bone spurs within a facet joint. Plain anterior-posterior (front-back), lateral (side view), and oblique (off-angle) x-ray films are typically used.
- MRI scans may be used for assessing the spine and its soft tissues, such as the discs and nerve roots. These scans may also help distinguish a chronic condition from an acute problem in certain situations. In analyzing a spine with a history of previous surgery, MRI’s are usually performed after a contrast dye is injected to better view blood flow in the region being studied.
- CT scans are helpful in viewing hard tissue, such as bone.
- SPECT scans are commonly used with a bone scan (nuclear imaging study commonly used to help find and track the extent of bone-related issues) or CT scan when viewing the intricate bones of the spine in order to see more areas and better details.
These tests may also help identify or rule out tumors and cysts in the lumbar spine.
Diagnostic facet joint block injection tests
Diagnostic blocks typically include injecting an anesthetic (numbing) and cortisone medication into the suspected facet joint. If the pain subsides during the anesthetic phase of the injection, a presumptive diagnosis of pain originating from the facet may be made.
While administering diagnostic injections, fluoroscopy (live x-ray) is used to guide the needle into the targeted facet joint. Contrast dye is usually used to enhance the visualization of the joint and to make sure that no vascular uptake (accidental entry of the medication into a blood vessel) occurs.
While a positive facet joint block injection may provide an accurate diagnosis of pain originating from the facet, 3 Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x these injections may also cause false-positive results. 4 Schütz U, Cakir B, Dreinhöfer K, Richter M, Koepp H. Diagnostic value of lumbar facet joint injection: a prospective triple cross-over study. PLoS One. 2011;6(11):e27991. doi:10.1371/journal.pone.0027991 To avoid false-positive test results, a double-block technique may be used. In a double-block technique, a second facet joint block injection is administered in the targeted facet(s) using local anesthetics with different durations of action (such as lidocaine and bupivacaine). For a positive test result, the patient must have >80% pain relief for an appropriate duration with each anesthetic agent. 5 Bartleson JD, Maus TP. Diagnostic and therapeutic spinal interventions: Facet joint interventions. Neurol Clin Pract. 2014;4(4):342‐346. doi:10.1212/CPJ.0000000000000044 , 6 Manchikanti L, Pampati S, Cash KA. Making sense of the accuracy of diagnostic lumbar facet joint nerve blocks: an assessment of the implications of 50% relief, 80% relief, single block, or controlled diagnostic blocks. Pain Physician. 2010;13(2):133-43. Available from: https://pubmed.ncbi.nlm.nih.gov/20309379/
Over time, disorders of the lumbar facets may affect the entire motion segment, causing varied symptoms in the lower back, hip, pelvis, abdomen, and/or leg. Once the facet joint disorder is diagnosed, a structured treatment approach for the specific condition (such as facet arthritis, fracture, or dislocation) is formulated. Both nonsurgical and surgical treatments are used to treat facet joint disorders.
- 1 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009.
- 2 Richard Field, Douglas Keene, Salahadin Abdi. Radiofrequency Treatment. In: Smith HS. Current Therapy in Pain. Elsevier Health Sciences; 2009.
- 3 Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x
- 4 Schütz U, Cakir B, Dreinhöfer K, Richter M, Koepp H. Diagnostic value of lumbar facet joint injection: a prospective triple cross-over study. PLoS One. 2011;6(11):e27991. doi:10.1371/journal.pone.0027991
- 5 Bartleson JD, Maus TP. Diagnostic and therapeutic spinal interventions: Facet joint interventions. Neurol Clin Pract. 2014;4(4):342‐346. doi:10.1212/CPJ.0000000000000044
- 6 Manchikanti L, Pampati S, Cash KA. Making sense of the accuracy of diagnostic lumbar facet joint nerve blocks: an assessment of the implications of 50% relief, 80% relief, single block, or controlled diagnostic blocks. Pain Physician. 2010;13(2):133-43. Available from: https://pubmed.ncbi.nlm.nih.gov/20309379/