A diagnosis of spinal infection is difficult to make early on in the course of the disease. If osteomyelitis is suspected, both diagnostic studies and laboratory studies will be conducted to make an accurate diagnosis. Sometimes, either an interventional radiological or surgical procedure may also be necessary to obtain a culture of the bacteria.
In This Article:
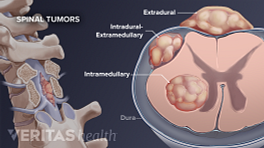
- Osteomyelitis, a Spinal Infection
- Osteomyelitis Symptoms
- Osteomyelitis Diagnosis
- Osteomyelitis Treatments
Diagnostic Studies

An MRI scan is a useful diagnostic tool to diagnose spinal infections.
The process of diagnosing a spinal infection usually starts with an X-ray. X-rays will usually be normal in the first 2 to 4 weeks after the infection starts. For changes to show up on an X-ray, 50% to 60% of the bone in the vertebral body needs to be destroyed. If the disc space is involved (discitis), the disc space may narrow and destruction of the endplates around the disc may be seen on the X-ray.
The most sensitive and specific imaging study for spinal infection is an MRI scan with enhancement with an intravenous dye (Gadolinium). The infection will cause an increase in blood flow to the vertebral body, and this will be picked up by the Gadolinium, which will enhance the MRI signal in areas of increased blood flow.
Older tests that are not as specific, such as bone scans, are still sometimes useful, especially if the patient cannot have a MRI scan. Bone scans are fairly reliable in determining if there is increased bone turnover in the spine, but cannot differentiate infection from tumor, trauma, or sometimes even normal degenerative changes.
Laboratory Studies
Blood cultures may help antibiotic treatment by identifying the causative organism.
Laboratory studies should also be obtained. Blood cultures may pick up the causative organism and help guide antibiotic therapy. Blood cultures are positive probably less than half the time, but when they are positive, they can be a very useful adjunct to guide the treatment (some bacteria are more sensitive to certain antibiotics than others).
Inflammatory markers can help indicate whether or not there is an infection. The erythrocyte sedimentation rate (ESR) and the C-reactive protein (CRP) are the two best known markers for inflammation, and they will be elevated in 80% to 90% of patients with osteomyelitis.
Another common test for an infection is level of white blood cells, however the white blood cell count may be normal in up to 70% of patients with vertebral osteomyelitis.
If all of the above markers are normal, it is unlikely that the patient has an infection.
If any of these markers are elevated, it can also serve as a baseline, and subsequent tests of these markers will indicate whether or not the patient is responding to a particular therapy. If the markers fall during treatment, then the treatment is likely to be successful in eradicating the infection.
Surgery

A biopsy contains a sample of the infected tissue and is used to identify the causative microorganism.
Surgery is sometimes necessary to obtain cultures for diagnosis of which type of bacteria are the cause of the infection. A biopsy may be obtained by needle biopsy, using a CT scan to visualize the needle and guide it into the infection. On occasion, open biopsy may also be necessary for diagnosis.