The surgery is chosen to address and correct where that pain’s coming from, and either to remove those structures or stabilize and fuse those structures so that there’s no longer a reason for pain. And then the— obviously the surgeon has to decide which techniques are the best in his hands—which has he been trained for, which has he had the most experienced with. And most surgeons that are orthopedic or neuro—they’re doing a lot of spine surgery—usually have multiple approaches that they can fit to the individual patient because of their body confirmation, because of prior surgery—either in the abdomen or in the back—it may persuade the surgeon to choose an alternative route to get the same outcome.
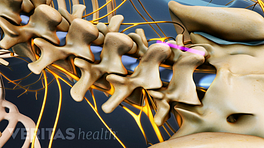
Spine fusion is a technique that spine surgeons use to immobilize one segment of the spine to the next segment of the spine. It can be done in the cervical region, the thoracic or chest region, or most commonly, really, in the lumbar spine or low back area.
And there are three main joints to the spine. The disc is actually a type of a joint. And then there’s two smaller joints on the backside of the spine. And classically most fusions have been done from the backside of the spine, making sure that those facet joints get fused as well as that whole segment. And there are two little arms that stick out from the side each vertebral body, those are called the transverse processes, and bone can be placed between those processes on the left down to the next level, on the right down to the next level, or down to the pelvis if you’re at the lowest level. And then that bone heals and immobilizes that segment so that you no longer should have pain from the motion of those joints, particularly the posterior joints.
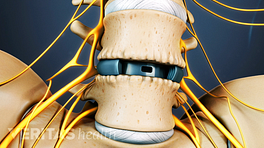
An interbody fusion can be done from multiple approaches. It can be done from the front, which is called an anterior spinal fusion, or interbody fusion, because you remove the disc material, you put bone into that evacuated space, and then the bone heals to the segment above and then the segment below. And that’s an extremely strong fusion because of the mass of bone you can get in and also because the anterior column of the spine is the portion of the spine that takes the most stress—eighty to ninety percent in a normal biomechanical situation. So that interbody fusion can be done from the front, as I’ve described, from the side, from a posterior-lateral, which is kind of obliquely off the midline, or from almost directly through the midline on each side. And that can help—when those fusions are done in the interspace, as well as out on the sides posteriorly, that’s when we get the highest fusion rates.
Articles Related to this Video: