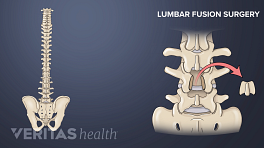
An anterior lumbar interbody fusion, called a ALIF, is designed to stop the motion at the symptomatic segment of the spine.
An ALIF is done in the lumbar, or lower, spine. Most commonly it is performed on the L4 through L5 or L5 through S1 segment at the bottom of the lumbar spine, as these segments are most likely to break down.
An ALIF is most commonly done to treat lumbar degenerative disc disease, in which a degenerated disc becomes painful. It may be done for other indications and may be combined with a posterior approach as well, if added stability is needed.
This type of fusion is unique as the surgery is done from the front, or anterior.
It starts with a 3 to 5-inch long incision on the left side of the abdomen.
Next, the abdomen muscles are retracted to the side.
The abdominal contents lay inside a large sack (the peritoneum) that is then retracted to the side, allowing access to the front of the spine without actually entering the abdomen.
The large blood vessels, called the aorta and vena cava, lay on top of the spine, so a vascular surgeon will usually be part of the surgery to move the large blood vessels to the side.
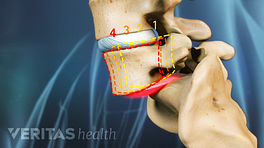
After the blood vessels have been moved aside, the disc material is removed.
Some type of implant, called a cage, is then inserted into the disc space. The cage helps restore more of the normal spacing in between the vertebrae, alleviating pressure on the nerve roots.
Bone graft is placed in the cage and sometimes in front of the cage.
Sometimes additional fixation is used by inserting screws through the cage.
If the patient's own bone graft is used, bone morsels are harvested from the front of the patient's iliac crest, or hip bone.
This is an additional surgical procedure that is done at the same time as the fusion surgery.
Synthetic bone graft options may also be used.
In the months following the surgery, the bone graft heals together through and alongside the cage, creating one long bone between the vertebrae and immobilizing that segment of the spine.
An ALIF may be combined with a simultaneous posterolateral fusion, with an approach from the back of the spine, if additional stability is needed to help ensure a successful fusion.
In This Article:
- Anterior Lumbar Interbody Fusion (ALIF) Surgery
- Potential Risks and Complications with ALIF Surgery
- ALIF (Anterior Lumbar Interbody Fusion) Video